
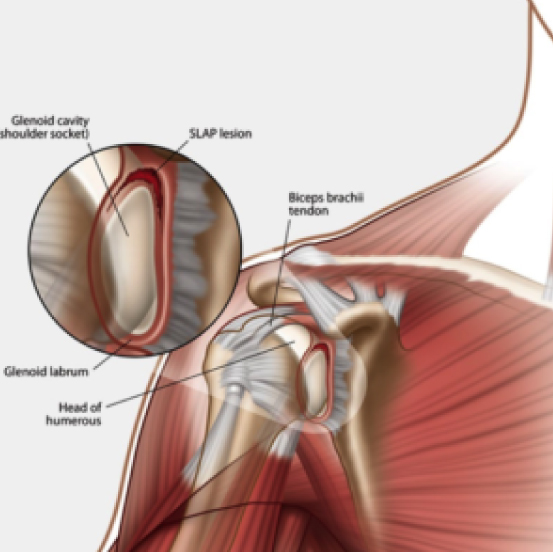
Shoulder Labral Tear
The labrum is a ring of cartilage that deepens the shoulder socket and maintains joint integrity by creating a “negative pressure seal.”
Labral tears most often occur from repetitive overhead activities, traumatic falls onto an outstretched arm or chronic instability, and present with clicking, catching or a deep ache—especially during external rotation or when lifting the arm.
At M Physio, we combine neuromuscular retraining to re-establish that suction seal with targeted strengthening of the rotator cuff and scapular stabilisers. We use specific mobility drills to gradually restore range of motion and reduce mechanical irritation.
Shoulder Partial (subluxation) or Full Dislocation
A true shoulder dislocation happens when the humeral head fully exits the glenoid, whereas a subluxation is a partial separation that often reduces itself.
These injuries typically stem from high-impact sports or trauma with the arm in an abducted, externally rotated position. Patients describe sudden pain, an obvious deformity at the time of injury, and afterwards a feeling that the shoulder “gives way.”
Our approach begins with early protection of the joint (often via a sling or brace), followed by careful reintroduction of controlled movement to prevent stiffness. Then, progressive activation of the deep stabilisers—particularly the rotator cuff and scapular muscles—to safeguard against repeat instability.

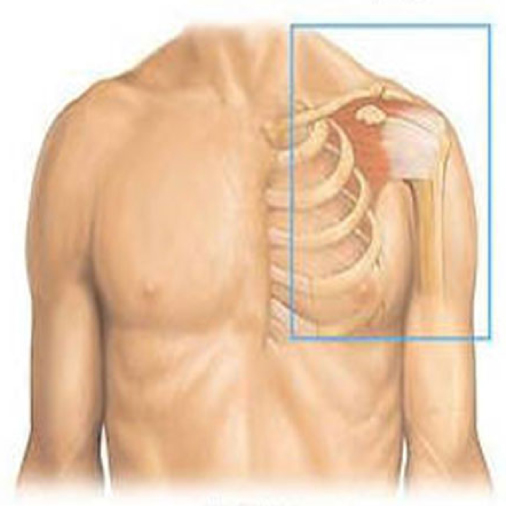
Shoulder Impingement Syndrome
Impingement arises when the rotator cuff tendons or subacromial bursa become pinched beneath the acromion, commonly from poor posture, repetitive overhead work or biomechanical imbalances.
Patients report a painful arc between about 70° and 120° of abduction and tenderness just below the acromion.
At M Physio, we free up the subacromial tissues with manual therapy, correct postural and scapular alignment and rebuild pain-free range. We often use targeted drills like wall slides and resisted rotations to re-establish smooth gliding under the acromion.
Shoulder Bursitis
When one of the shoulder’s fluid-filled sacs (bursae) becomes inflamed, it can swell and cause sharp pain with movement or when lying on the affected side.
We start physio with activity modification, ice or manual release to calm the inflammation. Then, as symptoms ease, introduce gentle joint mobilisations and soft-tissue stretches (for example, a door-frame–assisted anterior stretch) before returning gradually to everyday lifting and reaching.


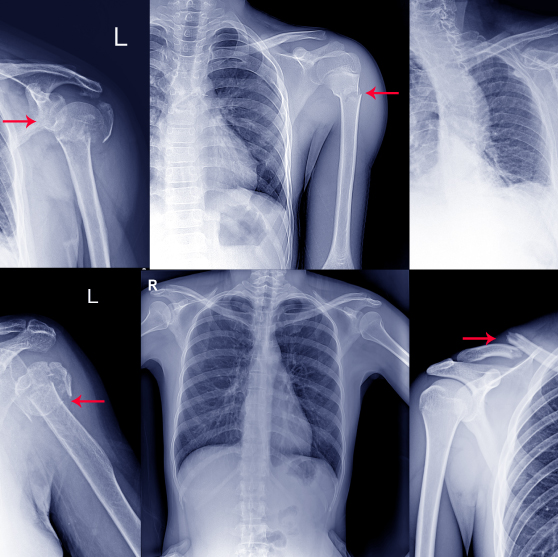
Shoulder Fracture
Fractures of the humerus, clavicle or scapula may require immobilisation or surgery, depending on the severity. Post-fracture rehabilitation is essential for regaining range, strength and function in the affected arm.
Initial rehab often involves lean forward pendulum exercises, where you let your affected arm hang and use gravity-assisted motion to gently swing and reintroduce shoulder movement. As healing progresses, we incorporate functional patterns, arm bent resisted external rotation, shoulder press and loaded carries under supervision.
Rotator Cuff Impairment
The rotator cuff is a group of four shoulder muscles that attach from your scapula (shoulder blade) to your upper arm bone (humerus).
Their main role is to keep the ‘ball’ of the humerus in the middle of the ‘socket’ on the scapula. These rotator cuff muscles also help to move the shoulder joint. Rotator cuff injuries can cause these muscles to get irritated, strained or torn. This can be a source of pain and dysfunction at the shoulder joint.
Our rehab protocol emphasises initial load management and pain relief, then moves into progressively challenging cuff-specific strengthening and control drills to rebuild muscle coordination and tendon resilience without overloading the healing tissue.

Frozen Shoulder
Frozen shoulder is characterised by progressive stiffness and limited range of motion, often affecting individuals aged 40–60. It progresses in three phases: freezing, frozen, and thawing. Early signs include difficulty with shoulder flexion, rotating the arm or reaching overhead.
At M Physio, treatment evolves with the stage of the condition:
- In the freezing stage, we focus on pain relief and maintaining available range with gentle stretch routines (e.g., pendulum exercises).
- During the frozen stage, more structured shoulder exercises such as wall walks, pulley work and external rotation are introduced.
- The thawing phase involves progressive strength-building and return-to-function planning.
Common Exercises for Shoulder Rehabilitation
Below are the core exercises we draw on across all shoulder conditions. Your physiotherapist will select and tailor these movements based on your diagnosis and stage of healing. Ensure you seek professional advice from a shoulder physiotherapist before attempting exercises.
Pendulum Swings
Lean forward, supporting yourself with your uninjured arm on a table or chair. Let the affected arm hang straight down and gently sway it in small circles or back-and-forth. Using gravity-assisted motion to restore early range without active muscle contraction is a common technique.
Band-Assisted Stretching
Flexion & Abduction:
Anchor a resistance band at hip height. Hold the band with your affected arm and walk backward until you feel a gentle stretch as you raise the arm forward (flexion) or out to the side (abduction).
External Rotation:
With your elbow bent at 90° and tucked into your side, hold the band and rotate your forearm away from your body.
Resistance Band Rows:
Anchor a band at chest height. Grasp with both hands, hinge forward slightly, and pull elbows back—squeezing shoulder blades together. This aims to strengthen mid-back and scapular stabilisers to support shoulder function.
Wall Slides and Walks
Stand facing a wall with your elbow bent and forearm against it. Slowly “slide” your arm upward along the wall, or walk your fingers up the wall, keeping contact and maintaining good posture, then lower under control. Wall slides improve pain-free overhead mobility and scapular control.
Pulley-Assisted Elevation
Using an overhead ceiling pulley system (or a towel draped over a door), grasp one end with your uninjured arm and gently pull to raise your affected arm. The purpose of this exercise is to promote smooth elevation through controlled assistance.
Eccentric Lowering Drills
Lift your arm to shoulder height (or overhead) using both arms or assistance, then lower it slowly (3–5 seconds) under the weight of the arm or light resistance. This exercise builds tendon resilience and muscle control.
Loaded Carries & Functional
Once basic strength returns, carry a light weight at your side, walking short distances while maintaining upright posture. Progress to overhead carries or presses as instructed. This exercise bridges rehab to real-world tasks, sports or job demands.
When to Seek Help for Shoulder Conditions
Shoulder pain that persists beyond a few days, worsens with movement, disturbs sleep or causes weakness in the affected arm should be assessed promptly. If you notice a sudden loss of motion or experience severe pain after trauma, early intervention can reduce complications.
Physio For Shoulder Pain - FAQ
Will my shoulder pain go away?
In most cases, yes — particularly when the correct diagnosis and an individualised treatment plan are in place. Many causes of shoulder pain, such as rotator cuff tendinopathies, bursitis and impingement, are highly responsive to physiotherapy. Your physiotherapist will assess the mobility, strength, posture and movement mechanics of your affected shoulder, then tailor a program to address underlying issues.
Treatment may include a combination of hands-on therapy, shoulder exercises, and functional re-training. Early intervention, load management and consistency with your program are key to restoring overall shoulder health and preventing recurrence. If your shoulder pain stems from more complex structural damage or systemic conditions, your shoulder physiotherapist may refer you for imaging or specialist input to support the best outcome.
Can physiotherapy treatment help with rotator cuff tears?
Yes — physiotherapy is often the first-line treatment for both partial and full-thickness rotator cuff tears. Even in cases where surgery is required, pre- and post-operative rehab is essential for improving strength, control and overall recovery.
A targeted program may include:
- External rotation strengthening (starting with the elbow bent at the side, then progressing to more dynamic patterns)
- Exercises like resisted shoulder abduction and arm straight forward raises
- Movement retraining and pain-relieving manual therapy
- Postural correction and scapular stability drills
Whether the injury occurred traumatically or over time, structured rehabilitation helps restore shoulder function, reduces pain and may help you avoid surgery altogether.
Is my shoulder pain serious?
Shoulder pain varies in severity and cause. While most cases are musculoskeletal and respond well to physiotherapy, some situations require medical attention. If your pain was caused by significant trauma (e.g. a fall or car accident), is accompanied by weakness in the affected arm, night sweats, unexplained weight loss, or severe pain that doesn’t improve with rest, it’s essential to seek a thorough assessment. Chronic pain following dislocation or labral injury may be a sign of underlying shoulder instability, which is best managed early through physiotherapy.
Fortunately, most shoulder complaints we see at M Physio are non-surgical and resolve with structured care. Your physiotherapist will screen for warning signs and refer you for imaging or medical input when appropriate.
Do I need a scan for my shoulder pain?
In many cases, no. Shoulder pain is often best diagnosed through a detailed clinical examination rather than immediately relying on imaging. Your physiotherapist will use a range of movement and resistance tests to assess the shoulder’s function, stability and strength.
If a scan is required, it may be due to:
- Suspected fracture (following trauma)
- Concerns about labral or tendon tears
- Lack of improvement after consistent rehab
- Screening for systemic conditions
If you already have scans, bring them along — we’ll review your results, correlate them with clinical findings and use that information to design your treatment plan.
What should I avoid while recovering from shoulder pain?
Depending on your diagnosis, you may need to avoid:
- Overhead or shoulder height movements in the early stages
- Lifting heavy objects with the injured arm
- Sleeping on the affected shoulder
- Movements that trigger symptoms, such as external rotation or fast, uncontrolled actions
Your physiotherapist will give you clear guidelines around what to avoid and when to safely reintroduce movements. For example, early rehab for impingement or bursitis may focus on gentle pendulum exercises with your affected arm hanging, before progressing to resisted shoulder flexion or abduction exercises in a supported starting position.
How long does it take to recover from shoulder injuries?
Recovery time depends on the type and severity of the injury. Here are general timelines:
- Minor sprains or overuse issues: 2–6 weeks
- Moderate injuries (e.g. tendinopathy, bursitis): 6–12 weeks
- Frozen shoulder: 6 months to 2 years (with different phases)
- Post-surgical rehab: 3–6 months, depending on procedure
Compliance with your home program — including daily mobility work, strength exercises and postural retraining — will accelerate recovery. Gradual progressions taught, such as slowly raise, slowly lower and slowly return movements, help ensure tissues adapt without overload.
What exercises can help relieve shoulder pain?
At M Physio, we prescribe exercises for shoulder pain that are safe to your specific presentation. These often include:
Gentle stretches for the posterior capsule or pec muscles
- Pendulum exercises with your arm bent or affected arm hanging
- Resistance band work for external rotation and scapular control
- Wall slides, pulleys or active-assisted shoulder flexion
- Functional drills to rebuild strength at and above shoulder height
Each exercise is taught with an appropriate starting position, and we monitor your form to ensure correct muscle activation and safety. Movements are often prescribed with cues like slowly raise and slowly lower to emphasise control.
What should I expect during my first physio for shoulder pain session?
Your first physiotherapy session at M Physio is designed to provide a clear diagnosis, a treatment roadmap and assurance. We take a comprehensive and personalised approach to understanding what’s driving your shoulder pain and how best to treat it.
Here’s what the initial session typically involves:
- Detailed Assessment
Your physical therapist will begin by taking a thorough history of your symptoms — including how the pain began, what movements trigger it and how it impacts your daily life or activities. We’ll also ask whether your affected arm or injured arm has any previous injury history or recent trauma. - Physical Examination
This involves assessing your posture, joint mobility, muscle strength and shoulder function through a series of guided tests. Movements like shoulder flexion, external rotation and shoulder abduction will be carefully evaluated. These movements help us pinpoint restrictions and pain generators. - Diagnosis & Education
Once we’ve identified the likely cause of your symptoms — whether it’s impingement, bursitis, rotator cuff injury or another condition — we’ll explain it clearly and answer any questions. We’ll also advise whether imaging is necessary and discuss your prognosis. - Individualised Treatment Plan
Your physiotherapist will tailor a plan that may include hands-on treatment, postural re-training and a progressive exercise program. You’ll often begin with safe movements during the session, such as:- Light banded external rotation work in a stable starting position
- Supported active-assisted shoulder exercises
- Instructions on how to slowly raise and slowly lower your arm with control
- Pain-relieving strategies to use at home
We also educate you on safe activity modification — such as avoiding repetitive overhead work or sleeping on the affected shoulder — and how to protect your overall shoulder health during recovery.
By the end of the session, you’ll know exactly what’s happening, what to do and what the next steps look like.
100% Money Back Satisfaction Guarantee*
Book in an appointment to see a physiotherapist for shoulder pain today Book An Appointment
*T&Cs apply